Articles
Transportation for Seniors in a Rural Community:
Can the Nursing Home Play a Role?
Abstract
In New Brunswick, a large percentage of the population is made up of older adults living in rural communities. This situation presents a number of challenges, particularly in terms of transportation. This paper describes a pilot project in a small rural community in New Brunswick in which a shuttle bus belonging to a long-term care facility was used to provide transportation for older adults living in the community. Both interviews and standardized quantitative measures of life satisfaction and depressive symptoms were used to measure quality of life with older adults who used the bus (n = 8) and older adults who did not use the bus (n = 17). Interviews with the bus drivers and program coordinators, as well as observations of a bus trip were also carried out. Bus takers were found to have lower scores on many quality-of-life indicators than non-bus takers, and were very satisfied with the bus service. Recommendations for increasing the long-term viability of the initiative are addressed in the Discussion.
Résumé
Au Nouveau Brunswick, une grande proportion de la population se compose d’adultes plus âgés qui vivent dans des collectivités rurales. Une telle situation pose un certain nombre de défis, notamment quant au transport. Le présent article expose un projet pilote d’une petite collectivité rurale du Nouveau Brunswick dans laquelle un bus-navette appartenant à un établissement de soins de longue durée a été utilisé pour transporter les adultes plus âgés qui vivent dans la collectivité. À la fois les entretiens, les mesures quantitatives normalisées de satisfaction à l’égard de la vie et les symptômes dépressifs ont été utilisés afin de mesurer la qualité de la vie des adultes plus âgés qui utilisaient le bus-navette (n = 8) et de ceux qui ne l’utilisaient pas (n = 17). Des entretiens avec les chauffeurs et les coordonnateurs du programme ont été effectués et des observations ont été recueillies au cours d’un trajet en bus-navette. Les personnes qui adoptaient ce moyen de transport présentaient des résultats plus faibles quant à de nombreux indicateurs de la qualité de vie que les personnes qui ne prenaient pas le bus et elles étaient très satisfaites du service de bus-navette. Des recommandations en vue d’accroître la viabilité à long terme de l’initiative sont abordées dans la discussion.
1 In Canada, the population is aging, with the percentage of adults aged 65 and over reported to be 16.1% in 2015, and expected to increase to 20.1% by 2024 (Statistics Canada “Canada’s Population Estimates”). By 2038, it is expected that the percentage of older adults in New Brunswick and Nova Scotia will surpass 30% (Statistics Canada “Population Projection”), due in part to younger people leaving eastern Canada in search of jobs (Willbond). Moreover, in New Brunswick, 40% of older adults live in areas defined as rural (Labour Market Analysis Directorate of Strategic Services, Atlantic Region). Rural living presents a number of challenges for older adults, and one of the primary challenges is transportation. In the present paper, we begin with an overview of the research addressing the links between transportation and quality of life for older adults in rural areas. Second, we describe a pilot project in which a long-term care facility in New Brunswick offered a new transportation option to the older adults in a small rural community, and we explore the impact of this initiative on the quality of life of older adults in this community.
2 Quality of life is a complex concept that includes physical and mental health, emotional well-being, and opportunities for social engagement (World Health Organization 1). A number of studies have focused on comparing the quality of life of older adults in rural and urban areas. While some researchers have found few differences in terms of health measures (e.g., Borders et al. 71), other have found that rural life is associated with higher risks for chronic conditions, and limited functioning in terms of activities in daily living (Baernholdt et al. 344; Keating et al. 330). Access to medical attention is a key link between health and transportation (Bacsu et al. 144; Kerschner 185). And limited transportation has frequently been found to be a barrier to healthy aging in place (e.g., Davey 60; Mattson 711). There have been consistent reports of a rural disadvantage in the availability, accessibility, and adequacy of health and social services, particularly for older adults (Krout and Bull 21), people with low incomes, and those with chronic diseases (Mattson 714). Moreover, these problems are exacerbated as health services are being increasingly consolidated in urban areas (Bacsu et al. 145).
3 Few studies have compared urban and rural communities on the frequency of mental illness in older adults. When such studies are carried out, it is frequently found that geographical area is not a significant factor (e.g., Bergdahl et al. 574), although some studies find that older adults in urban communities have higher rates of depression (Evans 432; Wang 23), and others find that mental health is more compromised in rural older adults (Milne et al. 483; Sharkey and Bolin 82). One possible explanation for the rural advantage that is sometimes found may be the presence of social support, with rural older adults in some studies reporting more frequent social interactions than those in urban areas (Evans 433). Clearly, community characteristics play an important role in predicting older adults’ well-being (Menec and Nowicki 11).
4 The relationship between opportunities for social interaction and emotional well-being highlight the importance of transportation in the lives of older adults in rural settings. For example, Banister and Bowling (1909) studied a sample of rural older adults in Britain and found that those with access to a vehicle attended more social events, and rated their quality of life higher. For those who did not have a vehicle, the number of social activities attended was correlated with ratings of local transportation options.
5 To understand the role of transportation in the emotional well-being of rural elderly, it is important to make a distinction between trips perceived as optional (e.g., social engagements, special occasions, non-food shopping) and trips perceived as non-discretionary (medical appointments and food shopping). Hanson and Hildebrand (982–98) used GPS technology to track older New Brunswick drivers over a few days, and subsequently interviewed these drivers regarding the purpose of the trips. The drivers reported that over a third of the trips taken would simply not occur at all if their car was not available. Only in the case of non-discretionary trips such as medical appointments and some shopping would they have been willing to ask friends and neighbours for a ride. The authors also pointed out that it was not clear whether family and friends would be able to meet even those limited transportation needs if the situation arose (989).
6 Davey (51) examined how older adults function without a car in New Zealand and also concluded that access to non-medical appointments was limited when older adults in rural areas do not have access to a car. Even when family was nearby, all transportation needs were not met (61). Older adults were uncomfortable asking for rides from friends and acquaintances (61) and were unwilling to ask even family members for transportation except for medical care and food shopping (61). Although taxis were sometimes used when medical emergencies were present, their use was limited because of cost (58). Thus, transportation for pleasure outings, for special occasions (reunions, funerals), and for special shopping (sales, seasonal fruits and vegetables) were likely to be unavailable (Davey 58). Mattson made similar conclusions in a study carried out in the American midwest, pointing out that transportation was particularly challenging for adults over 75 (712) and for rural elderly (714). Indeed, Mattson found that transportation options were so limited in rural areas that many older adults had moved to more urban areas for this reason (714).
7 Providing alternative forms of transportation for older adults residing in rural areas has been described as very challenging. Mattson and Kerschner pointed out that given the limited population base, even if public transportation was available, its usefulness and sustainability was likely to be reduced due to limited funding, limited scheduling, the need for home pick-ups, the need for single-client transportation, the long distances between pick-ups, and the long distances to destinations (Mattson 714; Kerschner 188–96). Moreover the reduced connectivity in many rural areas limits the use of advanced technologies that could possibly address many of these issues.
8 In the present study, we tracked the implementation of a pilot project aimed at enhancing the transportation opportunities for older adults living in a rural community in south central New Brunswick. The long-term care facility in this community received funds from a federal agency to pilot a project in which the shuttle bus usually reserved for the residents of the facility would be made available to older community members once a week for a trip to the regional urban centre at no cost. Information regarding the prototype project was collected in two main ways. First, interviews and standardized quantitative measures were used with older adults in the community who chose to use the bus service, and a sample of older adults from the community who were not using the service. Based on the review of the literature, it was predicted that older adults using the service would have lower quality of life (i.e., life satisfaction, depression, and social engagement) than older community residents who have access to private means of transportation, but that these differences would be attenuated by participation in the program. In a second part of this study, observational measures and qualitative interviews were carried out with certain key stakeholders in order to evaluate the program and make tentative recommendations for its long-term viability.
Methods
Participants
9 Thirty participants from a rural community in New Brunswick were interviewed in the fall (September and November). There were four groups of participants: (a) eight older adults registered for the bus service (mean age = 72.5, SD = 11.0), (b) two bus drivers, (c) three program coordinators, and (d) seventeen older community residents who were not using the bus service (mean age = 70.5, SD = 8.2). (Five older adults who registered for the service part way through the study and two bus takers whose intake forms were not received by the researcher were not included in analyses.) Three bus takers (37.5%) lived in the community where the long-term care facility was located and five bus takers (62.5%) lived in rural communities in the surrounding area. This is in contrast to the participants who were not using the bus: sixteen lived in the targeted community (94.1%), and only one (5.9%) lived in the surrounding area. In February and March, six bus takers and thirteen non-bus takers were interviewed a second time. Participants who were lost to follow-up could not be reached and it was reported to us that many were travelling during this time.
Materials
10 The following standardized instruments were used with all of the older adults during telephone interviews. The Satisfaction with Life Scale (Diener et al.) is a 7-point, five-item scale determined to have favourable psychometric properties, with a test-retest reliability coefficient of .82 and a Cronbach alpha of .87. Example statements include “In most ways my life is close to my ideal” and “If I could live my life over I would change almost nothing.” Scores can range from 5 to 35, with a higher score indicating a higher level of life satisfaction.
11 The Depression in Old Age Scale (DIA-S) developed by Heidenblut and Zank asks participants to respond true or false to ten statements about depressive symptoms. Examples of statements include “I am feeling down” and “I am worried about the future.” In the first validation of the scale, it showed good internal consistency (Cronbach’s alpha = .84) and an acceptable correlation with a diagnostic criterion (r = .73, Heidenblut and Zank 43). Scores range from 0 to 10, with a high score indicating a high level of depressive symptoms.
12 The demographic survey used was developed for this study. Older participants were asked to provide their age, marital status, and information about where they lived. For bus takers, some of this information was provided by the intake form filled out by participants when they joined the program. For non-bus takers, this information was gathered during the telephone interview. During the telephone interviews, older adults were asked to rate their health compared to others their own age, and then to rate their disability, both on scales from 1 to 10, with 1 being very low functioning and 10 being very high functioning. Additionally, they were asked the following questions: (a) Do you currently drive? (b) Do you have a car? (c) How do you usually get to where you want to go? (e.g., food shopping, clothes shopping, medical appointments, visiting friends), (d) Are there desired trips that you are unable to take? and (e) Is transportation a limiting factor?
13 Older participants were also asked to evaluate the shuttle bus program. For participants who used the service, these questions included how many times and how frequently they used the service, whether they used the service alone, and how satisfied they were with different aspects of the service. Satisfaction was measured using a scale ranging from 1 (not at all satisfied) to 10 (very satisfied). They were also asked to name two things they liked and two things they did not like about the service. Older participants who did not use the service were asked questions about whether or not they currently have a driving licence and a car, how they see their lives in five to ten years, whether transportation and mobility are a source of concern for them when thinking about the future, whether their current transportation gives them independence, and whether they feel they have family and friends who can assist in the future with transportation needs. They were also asked questions including whether or not they knew of the bus service offered by the long-term care facility, and under what circumstances they would and would not use the service. During the second interview (in the winter), participants were also asked if the weather affected their access to transportation.
14 In addition to the surveys for older adults, evaluations of the program were gathered from the bus drivers and the program coordinators. First, the bus drivers were asked to fill out a form after each trip. Each week, the driver noted when the bus left the long-term care facility, how many older adults were on the bus, pick-up and drop-off points, and concerns or issues that arose on the trip. Second, at one point during the study, bus drivers were interviewed, and guiding questions were used to ask about riders’ behaviour during the trips, perceptions of the benefits of the program, and concerns regarding the long-term viability of the program. Third, the program coordinators were interviewed regarding how and why the program was initiated, and their perceptions of the strengths and weaknesses of the program.
Procedure
15 The shuttle bus service was advertised widely throughout the community, and older community residents were asked to call the long-term care facility to register for the program. When individuals registered for the service, the bus coordinator filled out an intake form with demographic and physical health status information via the telephone. Once the intake process was completed, these older adults were asked if they would be willing to be contacted to participate in a survey. If they agreed to participate, they were contacted by the researcher via telephone, and after informed consent was obtained, the telephone interview took place. At the end of the interview, participants were asked for permission to be contacted again in February or March to do a follow-up interview. Older community members not using the shuttle bus were recruited through church bulletins, posters at public locations, and invitation cards distributed to members of seniors groups within the community. We did not offer an incentive for individuals to participate in the study.
16 The shuttle bus drivers and program coordinators were contacted directly and asked to participate. Interviews with the drivers were carried out in person, and interviews with the program coordinators were carried out over the telephone. Finally, the second author travelled on the bus one day in October, and was present on the bus from the time it left the long-term care facility at 9 a.m. to when it returned approximately five hours later. The researcher observed how the service works, how older adults interacted with the driver and each other, how long was spent at each stop, what happened at each pick-up and drop-off point, and any challenges that occurred on the trip.
Data Analysis
17 All of the interviews were recorded. Participants’ responses to open-ended questions were transcribed and then coded independently by two researchers. Interrater reliability was 87%. Responses to qualitative questions were coded using content analysis, and frequency counts were determined. For the quantitative data (satisfaction ratings and normed scales) inferential statistics were carried out using SPSS.
Results
18 We present the results in three parts. In the first part, a description of the shuttle bus program is provided, including observations carried out by one of the authors. In the second part, we provide a description of the older adults who chose to use the bus, and compare them to a group of older community residents who chose not to access the bus rides. Finally, in the third part, we evaluate the program from the perspective of the users, non-users, bus drivers, and program coordinators.
Part 1: Describing the Shuttle Bus Program
19 According to interviews with the program coordinators, the goal of the project was to keep older community residents in their own homes. As one coordinator said, “I think that it’s intended to allow seniors to stay in their home as long as possible. It is a benefit to seniors, the government; everyone benefits.” The program began offering free weekly rides to older adults in July 2014, and was still in effect in March 2015 when the present study was completed. When not driving the bus, the two drivers worked in the long-term care facility, one as a resident assistant and the other as the activity director. Shuttle bus riders were picked up at home and were taken to a local town about thirty minutes away, or to the regional centre approximately one hour away. Stops included banks, pharmacies, stores, malls, and the grocery store. The service ran twenty-seven times during this thirty-week period with an average of 4.4 riders (SD = 1.79). The number of riders ranged from one (immediately before Christmas) to seven (three different trips in October and November).
20 As part of the present study, the second author spent a day on the bus during one of its routine trips in the fall. The bus left the long-term care facility at the usual time of 9 a.m. to begin picking up individuals at their homes. It took just under an hour and a half to pick up the riders for that day and arrive at the local town. There were six older adults, the bus driver, a special care assistant accompanying one older adult, and the researcher. One participant was in a wheelchair. It was observed that scheduling was a challenge. Each rider had called the program coordinator during the week to say that they wanted to take the bus that day, and knew that it left the long-term care facility at 9 a.m. However, riders did not know who else was riding the bus that day and because participants lived far away from each other, it was difficult for them to judge when the bus would arrive at their home. In some cases, the bus would have to wait outside a senior’s home, and in others the senior was standing by the side of the road waiting for the bus to arrive. On that day, one person was not at the expected meeting point at all and time was lost waiting for them. The researcher also observed that many bus riders lived down long winding roads, which would make pick-ups during the winter difficult.
21 Coordination was also a challenge in town where the bus made a number of stops. For example, only one participant went in to the pharmacy and everyone else waited in the bus. At other locations, such as at the mall, everyone would get off and agree on what time they would meet outside the bus again. Because some passengers did not return by the agreed time, some were left waiting for others. At the lunch hour, the bus riders had to choose between going to the final shopping point (in this case the grocery store) and getting lunch for the bus ride back at a fast-food restaurant. Some of the older adults on the bus mentioned to the researcher that they were uncomfortable on the bus. They complained about how bumpy the ride was, and the researcher also felt that the bus seemed crowded. The bus was designed to seat fourteen, but two rows of seats were removed to allow for wheelchairs. After the shopping was completed, there was not much space left on the bus because of all of the packages and groceries.
22 Despite these challenges, the older adults seemed happy and more engaged with each other as the day progressed. The bus driver was very friendly with the bus riders: She helped them get on and off the bus and would get off the bus at the stops and chat with the waiting bus riders. The researcher did note, however, that it was physically challenging for the bus driver to help load and anchor the wheelchair onto the bus.
Part 2: Describing the Users of the Shuttle Bus Program
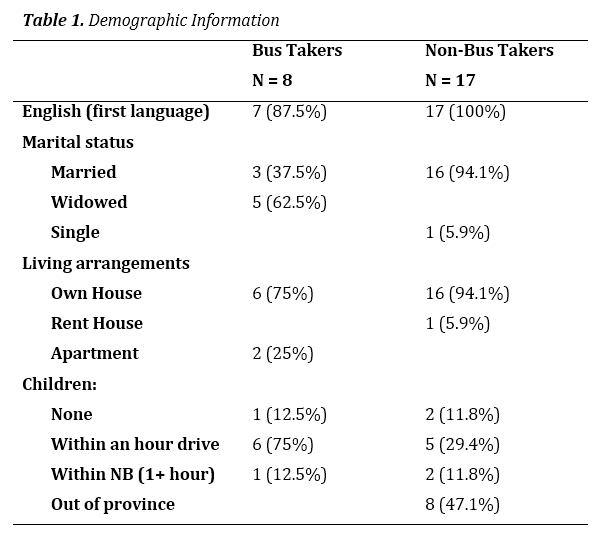
23 A summary of demographic information for bus takers and a comparison group of non-bus takers is presented in Table 1. In addition, both older adults taking the bus and a comparison group of older adults not taking the bus were asked to rate (a) their health and (b) their level of disability, both on scales ranging from 1 to 10 in the fall and winter interviews. Two separate 2 (season) × 2 (group) repeated-measures ANOVAs were carried out on these ratings. Non-bus takers (M = 8.39, SD =.26) had significantly higher health self-ratings than bus takers (M = 7.10, SD =.41), F (1,16) = 6.92, p = .02, η2 = .98. There was no significant effect of season on health, F (1,16) = .47, p = .47, η2 = .03, and season affected both groups similarly F (1,16) = .23, p = .23, η2 = .09. Non-bus takers (M = 8.92, SD = .34) had somewhat higher disability self-ratings than bus takers (M = 7.60, SD =.55), F (1,16) = 4.19, p = .06, η2 = .21. Neither the season factor (F (1,16) = .09, p = .77, η2 = .005) nor the interaction were significant (F (1,16) = .09, p = .77, η2 = .005) on this measure. Older adults in both groups were asked how frequently they went to medical appointments. Two participants reported a few times a month, and the rest reported a few appointments a year. When asked about health conditions, the most frequently listed condition was diabetes (25% of bus takers and 17.6% of non-bus takers).
24 Participants were given the Depression in Old Age Scale, and scores indicated that for the bus takers, scores increased from the fall (M = 1.67, SD = 1.5) to the winter (M = 1.83, SD = 1.46). A similar shift occurred with the non-bus takers (fall, M = .54, SD = 1.13; winter, M = .85, SD = 1.6). A repeated-measures ANOVA showed that this increase across the seasons was not statistically significant (F(1,17) = 1.35, p = .26,η2 = .07). The group effect was not significant, although the fairly large effect size suggests that with a larger sample, a significant finding could have emerged showing higher levels of depressive symptoms in the bus takers (F (1,17) = 2.82, p = .11, η2 =.14). There was no interaction (F (1,17) = .12, p =.73, η2 = .007). Scores on the Satisfaction with Life Scale did not differ meaningfully across the groups or the seasons; they ranged from a low of 27.8 (SD = 4.66) for the bus takers in the winter to a high of 29.15 (SD = 3.29) for non-bus takers in the fall.
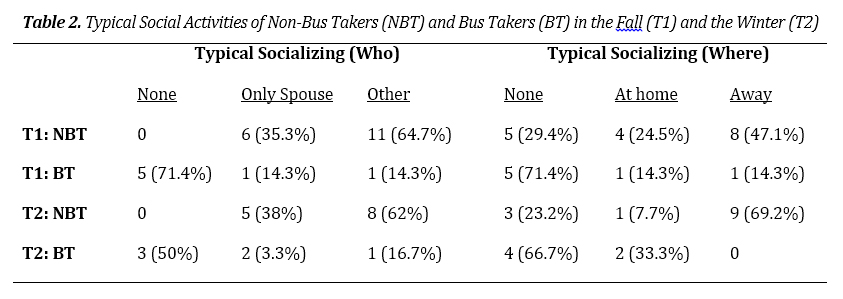
25 Following the recorded telephone interviews, the answers to the “typical day” question were transcribed and coded for types of socializing. These results are shown in Table 2. Chi square tests were conducted at Time 1 (fall) and Time 2 (winter). Non-bus takers have more social interaction overall, and more varied social interaction than the bus takers, both at Time 1, χ2 (2, N = 19) = 7.98, p = .02, and Time 2, χ2 (2, N = 19) = 8.27, p = .02. There was no significant difference found in where the two groups visit at Time 1, χ2 (2, N = 24) = 3.72, p = .15, but in the winter, non-bus takers have more outings than bus takers, χ2 (2, N = 19) = 7.98, p = .02). Similar findings were obtained when we counted the number of different activities reported in response to the question “What do you do for fun?” A repeated-measures ANOVA showed that non-bus takers (M = 3.39) overall reported more activities than bus takers (M = 1.75), F (1,17) = 10.39, p = .005, η2 = .38; season had no significant impact, F (1,17) < .01, p = .95, η2 = 0, and there was no significant interaction, F (1,17) = 2.25, p = .15, η2 = .12.
26 Open-ended questions asking participants to describe a typical day also suggested group differences, namely that bus takers had more limited scope for social engagement. Non-bus takers would usually describe days that were quite filled with activities, chores, and opportunities to socialize. For example, one non-bus taker described a typical day as “pretty busy and involves volunteering, working every Monday, Bible study, cross-country skiing, or the singing group.” In contrast, bus takers often listed fewer activities and their days often involved less socializing. For example, one bus taker said, “Just sit rocking my chair in the wintertime. There is nothing to do. Maybe some food prep and cleaning the apartment.” Indeed, when asked what they do for fun, a number of bus takers replied jokingly, “What is fun?” or “Fun doesn’t exist when you’re a senior.”
27 Participants in both groups were asked questions regarding their personal transportation options and typical transportation behaviours. As outlined in Table 3, there are a number of differences in these variables between the two groups. Although a surprisingly high number of bus takers own a vehicle or still drive, they are nonetheless more likely to have missed desired trips. (Unfortunately, the small sample precludes statistical tests of group differences.) When non-bus takers were asked open-ended questions concerning what conditions they would see themselves using the bus, the most common responses were if they didn’t have a car and were unable to drive. Many said that taking the bus would be inconvenient and would require planning and organization. During the winter interviews, 6 (50%) of the older adults reported that the weather resulted in their staying at home, but 9 (75%) reported that the weather did not have a significant impact on their ability to get around.
28 Non-bus takers were asked a series of questions about their thoughts and perceptions of transportation and mobility in the future. Their responses are outlined in Table 4. These results suggest that for the most part, these older adults had not reflected very much on the possibility of not driving in the future, and what alternative means of transportation they will use if they can no longer drive.
Part 3: Evaluating the Program
29 During the telephone interviews, the eight bus takers were asked to rate the bus program on a 10-point scale on variables of availability (M = 9.13, SD = .47), frequency (M = 9.2, SD = 2.12), comfort (M = 9.4, SD = 1.6), and friendliness of the driver (M = 10, SD = 0). Ratings were very high, and did not differ significantly when these questions were repeated during the winter interviews. It should be noted, however, that participants commented that during the winter, some trips were cancelled, and at least one individual mentioned not always feeling safe on the bus during the winter time.
30 In order to get the participants to further discuss their experiences on the bus, we also asked them to list two things they liked and two things they did not like about the bus. Relief from driving was the most common positive feature, followed by social reasons and being “good for me.” Independence, convenience, and cost were also mentioned. Participants had difficulty naming what they did not like about the bus. Two participants reported that the trip took too long or did not provide enough time for shopping, one reported that the trips were too infrequent, and one reported lack of comfort on the bus. When asked more open-ended questions about their reaction to the bus program, many of the bus takers had very positive reactions. One participant described the bus as having “dropped from heaven” and knowing that they can go once a week, and have the driver help carry bags to the door is great. Another participant described the program as “fantastic” and particularly helpful because many women in the community can’t drive.
31 Although reactions were generally positive, a few bus riders highlighted problems with the program. It was acknowledged that “the service is great for errands but not for appointments,” and some felt that it would be helpful if the bus ran more frequently or did not leave so early in the morning. It was also mentioned that the older adults were sometimes forced to sit in the back on the more uncomfortable seats because some seats in the front were occupied by a rider’s aid or companion. Finally, there were some participants who stated that they were taking the bus not because they needed to, but in order to ensure the program’s success. (Although at least one of these individuals admitted that she had not run errands in town at all during the three months preceding the beginning of the program.)
32 As a follow-up to the interviews with the older adults using the bus program, we also interviewed the two employees of the long-term care facility who drove the bus and the coordinators of the program. One of the bus drivers noted greatly enjoying the driving because it allowed her to interact with the program participants. The drivers felt that the bus riders were becoming more talkative as the weeks went by, and seemed to enjoy the social aspect of the bus trips. It was noted that the program “offers them freedom” and the opportunity to go shopping without having to ask friends and family for help.
33 The bus drivers also expressed concerns. They found it physically exhausting and stressful to help the riders who were in wheelchairs and needed a lot of support to get on and off the bus. From the perspective of the older adults, the drivers noted that many had found that (a) the timing (when they would be picked up) difficult, particularly at first, (b) some bus riders were frustrated by having to wait for others, and (c) some interpersonal conflicts were present between some of the older adults. The drivers also found it difficult to coordinate the timing when some riders wished to go to the larger (but farther) regional centre, but multiple and time-consuming pick-ups and drop-offs still had to be carried out.
34 Finally, from the perspective of the program in general, the drivers discussed both organizational and long-term feasibility concerns. In terms of day-to-day issues, the lack of clear guidelines on who could take the bus was problematic. For example, one senior used the bus to transport her severely physically handicapped daughter (who was not a senior), which led to complaints from some other riders on the bus. Also, some older adults with severe disabilities were not always accompanied by an aid or companion, which made the driver’s job much more challenging. In a few cases, older adults who had not filled out an intake form decided to go on the bus at the last minute, making it difficult for the driver to plan ahead, and contact information for emergencies was missing.
35 Overall, the biggest concern for both the drivers and the program coordinators was the long-term feasibility of the project. Even a few months before the pilot project was coming to an end, it remained unclear how funds would be raised to continue the project, and how unplanned costs such as bus breakdowns and continued awareness-building would be handled. Both the drivers and the coordinators were very aware that riders were pleased with the program, and that it served an important purpose in helping older community residents get to the bank, to the grocery store, and to the shopping mall. Coordinators, in particular, expressed an overall sense of optimism, and felt that the community was supportive, and had sufficient spirit and drive to make it happen.
Discussion
36 The goal of the present study was to describe the implementation of a transportation initiative in a small rural community in New Brunswick. Similar results to those found in rural communities in other parts of the world were obtained, namely that transportation is a challenge for many older community residents (Bacsu et al.; Davey; Kerschner 185; Mattson). As in Bacsu et al. (150), it was found here that many older adults who do not have their own personal vehicle rely on family or friends for transportation, and for some this is seen as a significant burden. As in Davey (55), having and driving one’s own vehicle was interpreted as a form of independence. Surprisingly few of the older community members who were still driving had considered their options if and when they could no longer drive. The ones who did consider this possibility either assumed that public transportation would be available, or planned to leave their home community and move to the city if they could no longer drive. It would be interesting in future research to follow drivers longitudinally when they cease driving, in order to better examine the complex interrelationships between the ability to drive and physical and mental health.
37 We expected that enhanced opportunities for transportation in the community would lead to an improved quality of life for older adults with limited transportation options. Nonetheless, we also expected that older adults who used this form of public transportation would have lower scores on quality-of-life measures (i.e., health, depression, life satisfaction, and social engagement) than older community members who used their own vehicles. Generally, this prediction was supported, though the standardized measure of life satisfaction did not yield statistically significant results, and no improvement was observed from the fall to the winter measures, perhaps because the scale is designed to measure overall satisfaction with life, not day-to-day changes. When we measured social activity occurring in descriptions of a typical day, clear contrasts were observed between drivers and bus takers. As in previous research (Banister and Bowling 109), those with access to a car are more likely to make it to social activities, which is a significant predictor of quality of life. Even with this small sample, and in a cohesive and supportive community, the impact of personal transportation was striking. Indeed, the fact that some of the bus takers explicitly said that they did not need to take the bus but chose to do so in order to support the program is indicative of the value older adults place on transportation initiatives such as this one. (It is also possible that for some people, this was a useful reason to accept a service that would otherwise have been perceived as threatening to their sense of independence.)
38 The users of the bus service gave very high satisfaction ratings across all dimensions of the service. Surprisingly, satisfaction did not change with time as people became accustomed with the service and the winter months set in. Of course, it is possible that riders felt that if they rated the program positively, it would be more likely to continue. It should be noted, however, that the open-ended comments, as well as the quantitative satisfaction ratings, were quite positive overall.
39 The two most successful outcomes of the program were the provision of social interactions and opportunities for shopping. Although most individuals travelled on the shuttle bus alone, most participants engaged with others during the trips. Riders described others on the bus as friendly, and it was observed that they spoke with one another. Opportunities for social interactions have been described as integral to healthy aging in place (Banister and Bowling).
40 Despite all of its strengths, there are challenges to ensure the ongoing success of the program. As has been noted elsewhere (e.g., Davey 58; Kerschner 196; Mattson 712, 714), the challenges to providing transportation services in rural areas are many. In rural areas, residents live far apart, and far from the departure point of the bus. In the present context, this meant that coordinating home pick-ups for multiple individuals was difficult to accomplish in a timely manner, and individuals were often left waiting in the cold, or standing by themselves on the side of the road without knowing exactly when the bus would arrive. Moreover, in order to allow for a meaningful amount of time to be spent in town, the outing was of a considerable length, and quite tiring for at least some individuals (i.e., from 9 a.m. to past 3 p.m.). Finally, while the service is set up well to help older adults carry out errands, it does not easily accommodate transportation for medical or other appointments. Thus, this type of program has to be perceived as only one part of the services rural communities need to offer in order to allow their residents to “age in place.” Indeed, as this study was ending, the community in question was attempting to put in place a companion dial-a-ride program for older community residents needing transportation to medical appointments.
41 The present study has many limitations. The small number of older community members who registered for the program limited our sample size, and a comparison group of older adults who were without independent transportation options but chose not to use the bus service was impossible to recruit. Additionally, participant retention for the longitudinal aspect of the study was challenging because a number of older adults went away for the winter months and could not be contacted for a follow-up interview. A second major limitation was the timeline for the project. The research project began as the bus service started to operate, and concluded as the pilot grant was concluding; however, to study the topic in depth it would be beneficial to have the project run over a number of years, rather than just over a few months. This would allow a better measure of the impact of the service on older adults’ well-being, and it would allow a longer period to assess how well the shuttle bus service achieved its goal of helping individuals stay in their home longer. Despite these limitations, this study is significant because there is currently very little research evaluating specific transportation interventions. There are a number of studies highlighting the need for transportation initiatives for older adults living in rural areas, and many communities have set up different types of programs, but there is a distinct lack of studies to evaluate the relative success of these types of interventions.
42 To conclude, we reproduce here a series of recommendations that were offered by the research team to the program coordinators with the goal of helping to ensure the long-term feasibility of the shuttle bus program.
- Government support. A discussion is needed at the local, provincial, and federal levels for transportation needs of rural older adults to be considered as an integral part of health and wellness services. This recognition of transportation, particularly in rural areas, as a key social determinant of health should lead to financial support for programs such as this one that help ensure that older adults in rural communities have access to all of the services that ensure their continued well-being in the community.
- Implementation of a membership fee. Although this would not be a popular option with current bus takers, it is likely essential for the program to continue. One model would involve charging a fee on a weekly basis for taking the bus. A second option is a membership fee. This would involve older community members paying for membership for six months or a year for the service. Although this may be more challenging for some of the potential users of the service than the week-by-week option, it allows the program coordinators to budget appropriately, and ensure that sufficient revenue is present to operate the service. Of course, payment waivers should be available for at least some individuals who are unable to pay the fee.
- Fundraising. Fundraising at the community level, support from private businesses in exchange for advertising, and other types of subsidies to the service are likely to be needed over and above user fees.
- Operating policies for riders. Policies should clearly outline who is to use the bus so that guests do not take up space on the bus and taking away from the experience of other adults in the community. Additionally, only those who have filled out bus intake forms should be allowed on the bus for liability reasons. It may also be necessary to limit the size and number of packages allowed on the bus to ensure the safety of passengers and driver.
- Operating policies for drivers. Policies outlining the role of the bus driver should also be put in place in order to ensure that employees can safely and comfortably continue to offer this service. Currently, the bus drivers are doing much more than driving the bus. They are helping with parcels, making lunch purchases for bus takers, and, more importantly, lifting heavy wheelchairs on and off the bus. Some programs in other communities require that passengers who need lifting out of the bus bring a companion.
- Carpooling. One of the major issues with the shuttle bus service is that three hours of the six-hour trip are spent driving considerable distances in order to pick up and drop off riders in surrounding areas. Some older residents who participate in the program are willing to drive from their home to the long-term care facility, but are unwilling to drive in the city. Older adults who are able to pick up other bus takers on their way to the bus should be encouraged to do so. Additionally, volunteers from the community could also provide rides to older adults to get to the long-term care facility at the beginning and end of the day, and there could be a social gathering at the facility while both the bus takers and community volunteers wait for others to arrive. This would save a lot of time riding the bus, and would allow more time in the city centre. This would also reduce the amount of fuel required for the trip.
- Recruitment and advertising. It is essential to continue advertising the service to ensure that all community residents who need the service know it exists.
- Consultation with bus takers. The present study identified many challenges and possible solutions by interviewing the older adults who use the shuttle bus service. Ongoing consultation with users of the service would be extremely helpful to the program coordinators.
Appendix
 Display large image of Table 2
Display large image of Table 2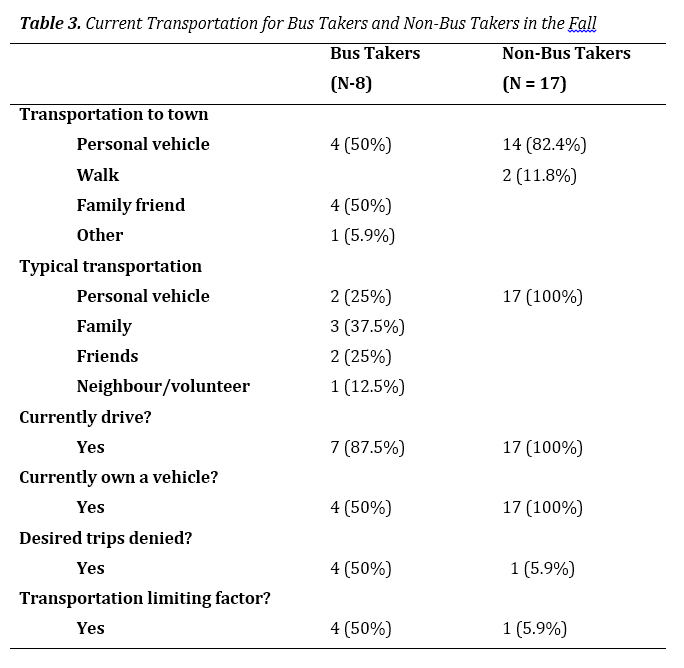 Display large image of Table 3
Display large image of Table 3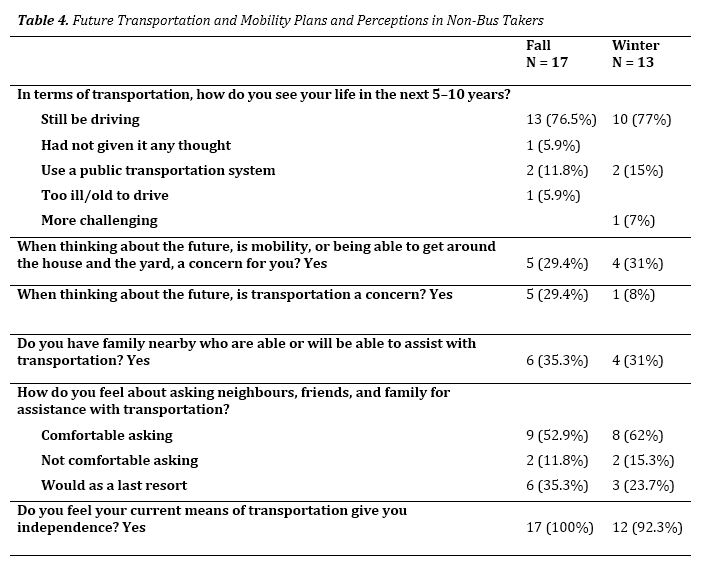 Display large image of Table 4
Display large image of Table 4The authors would like to thank Jodi Hall, John Shackleton, and the members of the board of directors of the long-term care facility for their support of this research project.