The Politics of Mental Health Care in Nova Scotia:
The Case of the Halifax County Hospital, 1940-1976
Judith FingardJohn Rutherford
Dalhousie University
1 AFTER THE SECOND WORLD WAR, significant changes occurred in the care of the mentally ill in Canada as the government moved toward the adoption of national health insurance. Reforms were encouraged by the introduction in 1948 of federal health grants channelled through the provinces to train mental health professionals, construct new facilities and support research. In return for the injection of federal funds, the mental hospitals controlled by the provinces were required to admit patients free of charge. Subsequently, mental hospitals were excluded from the provisions of the Hospital Insurance and Diagnostic Services Act of 1958, an exclusion that became more serious as the federal health grants were phased out. Some of the provinces – Ontario (in part), Quebec and Nova Scotia – eventually corrected this anomaly. Nova Scotia, which adopted hospital insurance in 1959, extended coverage to its mental hospitals in 1966 and 1967.1 The records of one of those hospitals, the Halifax County Hospital (HCH), the hospital that is the subject of this paper, indicate that the new government financing was implemented in halting, uncertain stages. While the hospital’s management and administration welcomed federally enhanced provincial funding for construction, drugs, staffing and programming, the fate of the patients depended on system-wide improvements that were slow in coming. Ultimately, it was the social-welfare legislation of the late-1950s and mid-1960s (also made possible by federal funding) as much as the health care reforms that determined mental health practice.
2 Each mental hospital in Canada experienced the political and economic changes of the post-war period differently and was influenced not only by federal and provincial policies but also by its location, staff, management and the composition of its patient population. All of these hospitals, however, shared certain key developments. Hospital practice was revolutionized by changes in treatment, especially by the transition to community care and the introduction of effective drug therapy. Prominent among the measures that led to the depopulation of the mental hospitals were the unlocking of doors, encouragement of short-term leave, introduction of new social therapies and rehabilitative programming, establishment of out-patient services, day-care and night programmes, access to sheltered workshops, initiation of support groups for ex-patients, and the provision of assisted-care living arrangements in foster or group homes.2 At the same time, the introduction in the 1950s of chlorpromazine as an anti-psychotic and in the 1960s of imiprimine as an anti-depressant heralded the replacement of the sedatives and crude physical treatments – insulin shock and psychosurgery – by effective chemical substances.3 These changes in psychiatric practice are what set this study of a post-Second World War facility apart from those of the asylum era, which have tended to capture the attention of social historians in Canada.4 Traditional institutional histories, which include the post-war period in their scope, have been left to local historians and former staff who have focused mainly on full-service psychiatric hospitals like the Waterford and the Brandon or on the 20th-century generation of active-treatment centres such as the Toronto Psychiatric Hospital.5 Some of the publications have been commissioned volumes with an emphasis on "progress" – Cahan’s history, for example, of the Douglas Hospital in Verdun – and those that mark an anniversary have been celebratory in tone.6 There is nothing celebratory about the story of the Halifax County Hospital.
Nova Scotia’s Mental Health Culture
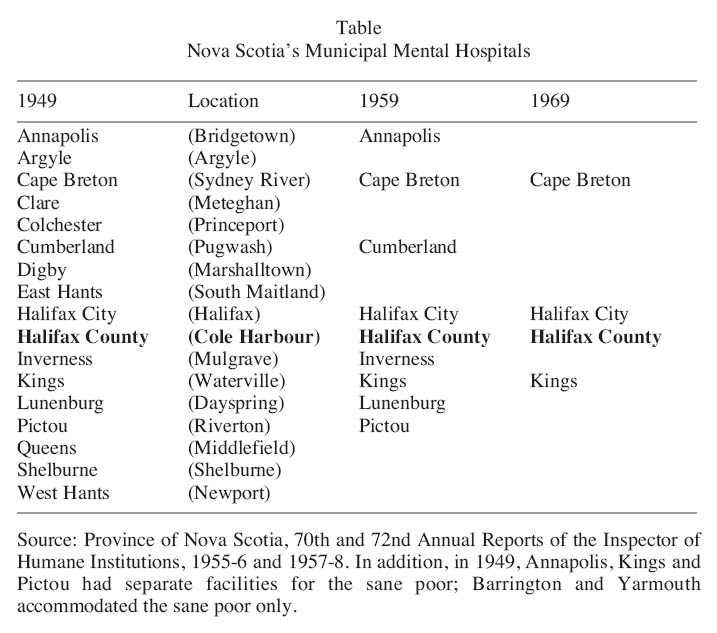
3 The specific course of a hospital’s development was affected by the particular mental health culture of the jurisdiction in which it was located. With the exception of Quebec’s religious institutions and Ontario’s long-lasting private asylum in Guelph, Canada’s mental hospitals were public.7 In Nova Scotia the public mental hospital system had a two-tiered structure that separated the care of the newly diagnosed sick from those assessed to be chronically ill by placing them, not in different wards or buildings, but in different hospitals. Unlike some provinces, which experimented with separating the two populations in the early-20th century by establishing acute-care hospitals, Nova Scotia’s first-tier, acute-care institution preceded the establishment of those hospitals devoted to the care of the incurable.8 This institution, the Nova Scotia Hospital on the Dartmouth side of Halifax Harbour, opened in 1858 and was owned and operated by the government of Nova Scotia.9 On the other hand, the second tier, comprising the custodial, chronic-care hospitals, most of which were established in the late-19th century, were funded and run by the municipalities. They consisted in the late 1940s of 17 municipal mental hospitals (designated county, district or town/city) located in 14 of the province’s 18 counties (see Table). The Halifax County Hospital in Cole Harbour, outside of Dartmouth, was one of them.
Table : Nova Scotia’s Municipal Mental Hospitals
Display large image of Table 1
4 In the late-19th century the aim had been to establish cottage hospitals for the mentally ill in their own communities but, with insufficient funding, most of them had become poor houses or closely associated with a poor house in a province, which had copied the British poor law more faithfully than any other Canadian province.10 Because the county and municipal homes and hospitals were small, isolated and lacked mental health professionals and social amenities, they were harshly criticized in a number of reports between the 1940s and 1960s. Accordingly, when Dr. Clyde Marshall was appointed Nova Scotia’s first director of mental health services in 1947, he set out to reform the mental hospitals and attracted almost universal support.11
5 In theory, the long-overdue inclusion of the second tier of Nova Scotia’s mental institutions within the provincial health-care orbit should have been a positive development for patients and staff. All of the hospitals stood to benefit from modernization – better buildings, professional rather than untrained staff, programming for patients and management accountability. In practice, however, each step forward was accompanied by two steps back. Some of the problems had to do with long delays on the part of a provincial government dependent on the new cost-sharing arrangements introduced by Ottawa. Other problems centred on the loss of local control when new bureaucracies became involved, the emergence of turf wars between the provincial departments of health and of welfare, and endless "nickel-anddiming" by all levels of government. The campaign to reduce the patient population provides a telling illustration of the fits and starts associated with changes in the 1950s and 1960s. Such reductions did not proceed in a smooth, linear fashion. Indeed, the evaluation of institutions by the department of health, which coincided with the classification of patients by the department of welfare, meant that when the Halifax County Hospital was assessed to be one of the best, its "catchment" area was expanded so that the department of health could use it to accommodate patients formerly housed in institutions that failed to meet the provincially imposed standards for mental hospitals. The Halifax County facility became an overcrowded hospital virtually paralysed by uncertainty as to its role in the "system".
6 As the Appendix helps to illustrate, the jurisdictional features of the Halifax County Hospital (and its companion institutions) were multi-layered in complexity and subject to change. The HCH buildings and land belonged to Halifax County. Although nominally the responsibility of the Halifax County Council, which oversaw its day-to-day operations by means of a management board both before and after the advent of provincial funding, the HCH was also supposed to be subject to provincial scrutiny through a variety of mechanisms. One was the annual inspection by the director of humane institutions, who reported to the provincial department of health. The inspector also had considerable responsibility for the admission and release of patients. Another check was a municipally appointed visiting committee that by the 1960s was required to report to provincial government authorities about the conditions it encountered. A third mechanism dates from 1958 when the provincial department of health began to provide partial funding for operations. One of the conditions was the requirement that the board include provincial appointees among its membership and ensure that a majority of its members be drawn from outside the municipal council, a regulation that continued in the 1960s under the Nova Scotia Hospital Insurance Commission (NSHIC), the body responsible for the national health insurance programme in the province.
7 The division between municipal and provincial responsibilities was not the only political aspect of the hospital’s administration because the HCH operated as a health, welfare and penal institution for the province. Its health services were increasingly brought under the control of provincial authorities both directly through the office of the director of mental health services in the department of health and indirectly through the medical administration of the Nova Scotia Hospital, which the director supervised. An additional administrative layer, represented by the NSHIC, was gradually introduced between the 1959 introduction of subsidized care in most general hospitals and the 1966 official financial takeover of the municipal mental hospitals by the commission. Provincial scrutiny meant that all increases in expenses desired by the municipality – including renovations and staffing – had to be approved by the authorities in Halifax. Until the municipal hospitals were covered by hospital insurance, most charges for patient care were billed to the patient’s district of settlement, a legacy of the poor law that had been eliminated at the Nova Scotia Hospital under the terms of the federal mental health grants. Welfare services were also subject to provincial oversight. As Nova Scotia’s welfare bureaucracy expanded to administer federal funding through the provincial Social Assistance Act of 1958, it became more involved in hospital operations as the authority for securing welfare patients (whether old, physically disabled or mentally challenged) alternative places to live either as residents in congregate homes or as boarders in foster or group homes in the community. Because of their eligibility for support under the Canada Assistance Plan of 1966, many post-mentally ill patients, discharged into the community, also came under the supervision of the provincial department of welfare. That department’s continued involvement – indeed its takeover of the Halifax County Hospital in the 1970s – was dictated by further provisions of provincial health and federal welfare legislation.
8 The third government department involved in the HCH and other mental hospitals was the provincial attorney general’s office, which was responsible for forensic psychiatric cases – especially the disposition of patients with criminal records confined under lieutenant governor’s warrants as either unfit to stand trial or not guilty by reason of insanity. These inmates were, in effect, wards of the lieutenant governor and detained at his pleasure. Some of these cases were remanded to the HCH. Regardless of their status, people deemed insane and committed to the Halifax County Hospital as transfers from the Nova Scotia Hospital would already have been certified by two medical practitioners. The non-warrant patients tended to be the outcasts of society, especially of their families. There were also direct admissions to the HCH, but they were supposed to be restricted to people – such as the senile and the retarded – who would demonstrably be unable to benefit from assessment and treatment in the acute-care facility. With the implementation of the Municipal Mental Hospitals Act in 1966, the grounds for committal of all patients became subject to regular review; voluntary admission, as an alternative to committal, was encouraged and judicial review to secure release was instituted.12
9 For the administration of the Halifax County Hospital we have identified five successive phases between its rebuilding in 1940 and its re-invention in the late 1970s as the Halifax County Regional Rehabilitation Centre: establishment, flux, modernization, catharsis and limbo.
The Establishment of the HCH (1940-51)
10 The Halifax County Home and Mental Hospital, built on a scenic, 200-acre site at Cole Harbour, accepted its first patients in 1940 when a new building was opened to replace the previous municipal poor law institution and asylum, which had burned down in 1929.13 The new HCH was largely custodial, with its patients and paupers drawn mostly from Halifax County. The institution was not, however, entirely divorced from new trends in psychiatric treatment. At the request of medical officer Peter Hebb, a general practitioner, the board – comprised of municipal councillors and the county warden – bought an electroshock machine. Electroconvulsive therapy (ECT) commenced in 1943, only a year after the sole university psychiatrist of the day and an avid proponent of ECT, Dr. R.O. Jones, had initiated this treatment at the Halifax City Home and the same year that the treatment was introduced at the Nova Scotia Hospital, where a full array of physical therapies was in vogue including insulin coma and lobotomies.14 Although the HCH was not designated by the provincial department of health as a therapeutic centre, the board’s eagerness to treat patients on its own initiative may have had the benefit of encouraging the attending physician to take a greater interest in the patients and to make the daily visits mandated by law.15
11 In this first phase, the only programming provided for patients consisted of labour in the hospital or on the hospital farm for a capable minority, occasional religious services and films shown once a month by the first recreational volunteers, members of a local Kiwanis club. For an institution of 260 patients, including about 65 indigents – undifferentiated between certified and uncertified, children and adults, tubercular and non-tubercular, but segregated by sex and class (there were paying patients) – the health-care staff consisted of only about 20 largely untrained attendants.16 In 1947, the year of the first courtesy visit by Clyde Marshall as provincial director of mental health services, the only registered nurses (RNs) at the HCH were administrators – the superintendent Edward V. Smith and his wife Vera, the matron – and the only physician, Peter Hebb, was employed at the hospital in a part-time capacity. Those patients transferred from the Nova Scotia Hospital, because of their presumed incurability, either suffered from organic brain disease or were "burnt out" from chronic psychosis (described by one informant as catatonics and simple schizophrenics).17 The Nova Scotia Hospital report for 1947, a typical year, reveals that its transfers to the municipal mental hospitals, including the HCH, for long-term (often life-long) custodial care equalled nearly one-third of the Nova Scotia Hospital’s admissions.18 The year 1948 saw a somewhat ominous change in the relationship between the Nova Scotia Hospital and the municipal institutions, when legal provision was made for patients held under lieutenant governor’s warrants as criminally insane to be among those transferred to municipal care.19
12 At the HCH, the attrition rate among the untrained, partially live-in staff who tried to manage the assorted population was extremely high. An in-service training programme for attendants offered in 1944 was not revived until 1954, probably because it was considered a poor investment in staff who would not stay.20 The county council, which operated the hospital with municipal tax funds, blamed the staff turnover on low wages – as low as $60 a month for ward attendants in 1950 – and on the remote location, which was not served by any form of public transportation.21 Since the municipal authorities always put the interests of taxpayers first, they were not inclined to favour improvements for the staff. Despite its striking lack of resources, the HCH was, according to Clyde Marshall, "the only municipal institution in the province worthy of praise", a comment which was more condemnatory of the other municipal institutions than complimentary of the HCH.22 Until the mid-1950s Marshall had no authority over the municipal institutions. They were subject to an annual inspection by Dr. J.J. MacRitchie, the province’s inspector of humane institutions, whose duties were governed by the provincial statutes of 1923 that dictated the management procedures for all the municipal mental hospitals.23 Nonetheless, Marshall’s appointment and the initiation in 1948 of the federal health grant programme were prophetic developments for the HCH.
A State of Flux at the HCH (1952-58)24
13 The scale of the hospital’s operation and the influence of the provincial government both increased during the 1950s. In 1952, as a result of overcrowding, a second building – constructed with the help of a federal-provincial hospital construction grant – was opened and the complex officially adopted the name "hospital" and dropped "home". Although at the time the funding under the new national health policy initiative was seen as a great coup, the resulting admission of more patients created even greater problems. While the available space was doubled, the number of patients was also doubled, peaking at 600 in 1955.25 And while more staff members were hired, they became vastly overworked as the expanded hospital was transformed into a dumping ground for severely and chronically ill bed patients – mental and physical – from numerous municipalities with inadequate or no facilities.26 Several of the small municipal institutions were closed after Marshall replaced MacRitchie as provincial inspector in 1955 and the slack had to be taken up by the remaining hospitals, which increasingly admitted residents from outside their own area. With a greater patient load at the HCH, staff turnover among the young, easily discouraged workforce was worse than ever. Of the 60 members on the nursing staff in 1954, for example, 34 had been hired that very year and 19 of the remaining 26 the previous year.27 Fully aware that the work was unattractive and that even the better competitors such as the Nova Scotia Hospital were having difficulty retaining staff, Superintendent E.V. Smith tried, largely unsuccessfully, to recruit in the poorer, more remote rural areas like Guysborough and Richmond counties.28 When he claimed to be losing his "best staff" in 1954, he secured from the county council salary increases averaging about 50 per cent for all the nursing staff and skilled trades people, but the better remuneration appears not to have halted the high rate of staff changes.29 Interestingly, however, at a time when most levels of government discouraged the employment of married women in the public service, the most reliable staff at the HCH were married women who assumed responsible positions in nursing, housekeeping, dietetics and occupational therapy.
14 Personnel policies, as much as low wages, discouraged retention. One board member claimed in 1953 that "living-in turns many prospective staff people away from the hospital".30 Staff living quarters afforded no social focus. Because of the lack of transportation, there was little opportunity for employees to go to town for a break. Moreover, since the staff quarters were not in a separate building, the employees were "never away from the sounds and smells of the hospital".31 The wife of the assistant superintendent between 1948 and 1959 served as ward attendant, dietitian to the bed patients and assistant to the medical officer during ECT sessions. She recalls that the hospital apartment in which her family first resided was on the main floor of the older building, beneath which was located the cell block where disturbed patients were locked away in solitary confinement until their behaviour improved. When her mother visited, she was frightened by the unearthly noises emanating from beneath the family’s lodgings.32
15 Given these circumstances, it was hardly surprising that drinking by both attendants and patients was frequently detected in the staff quarters and the wards. This was a major cause of dismissal of employees.33 Whatever their transgressions, staff (frequently misfits themselves and occasionally, in fact, ex-patients) were treated by management more like disobedient children than employees with rights. Indeed, employees’ "rights" (let alone patients’ rights) were not acknowledged. For example, the board claimed "a vacation is not a right but a privilege".34 Employee complaints and problems were dealt with on a case-by-case basis. With respect to injuries, it was not until 1960 that the HCH joined the provincial workers’ compensation programme. When a staff member broke an arm in the kitchen in 1954, payment of her hospital bill was at the discretion of the board, which in this case accepted the liability.35 For patients, too, the work could be dangerous. One young woman who worked in the laundry got her arm caught in a mangle and was badly injured.36
16 Low salaries and paternalistic employment practices were bad enough, but long hours and unfulfilling duties also contributed to the continued shortage of staff. In June 1952, after losing 12 of his employees or about 15 per cent of his workforce, Superintendent Smith admitted that a 10-hour day as well as working with insane patients scared off most job-seekers.37 With a total of 80 hard-pressed staff (nursing and others), it is not surprising that patient labour became essential to the operation of the hospital. Indeed, in 1954, shortly after a programme of occupational therapy was first mooted by the hospital’s watchdog visiting committee, the superintendent claimed such a programme was not needed because those patients who were able to work already did so in the hospital building or grounds.38
17 The decade of the 1950s was nonetheless an exciting time therapeutically. The single most significant contribution for improving staffing and prospects for patients came from the introduction of the new psychotropic drug, chlorpromazine. Developed in France in 1951 and introduced to Canada in 1953, it revolutionized institutional drug therapy for schizophrenic conditions, the treatment of which had formerly relied on the use of debilitating sedatives.39 Chlorpromazine was first used at the HCH in 1955. Dr. Frank Malcolm, the hospital’s ex-army medical officer, soon reported that patients in the disturbed wards who had been "stark raving maniacs . . . have become almost sane people through the administration of largactil [the trade name for chlorpromazine] in proper quantities", while adding "the possibilities of improvement are amazing and practically unlimited in most types of patients".40 The need to administer, calibrate and monitor these potentially dangerous drugs (too large a dose can produce Parkinson-like symptoms) resulted in Malcolm being made a full-time employee in 1956.41 Because the new drug therapy was expensive, both in terms of the drug itself and the additional medical and nursing requirements, the hospital asked for financial help from the province.42 This request gave Marshall the leverage he needed to encourage the HCH over the next few years to qualify for approval as a provincially administered psychiatric institution under his plans for upgrading the standards of the municipal mental hospitals. In the process, however, it became apparent that provincial bureaucratic procedures took far longer to produce results than the municipal ones and that civil servants, not hospital administrators, now called the shots. The HCH was made to wait for provincial approval of every improvement its board sanctioned. For instance, authorization to appoint an occupational therapist took over a year of negotiation in 1956-7.43 Meanwhile, changes in provincial legislation in 1954 gave the province more control over the admission and discharge of patients in the municipal hospitals and provided the first evidence that rehabilitation might become part of mental health services through the enactment of a provision for trial periods of release of up to 90 days.44 Excluded, like all mental hospitals across Canada, from the cost-sharing arrangements of the federal hospital insurance scheme that came into effect in Nova Scotia in 1959, the municipal mental hospitals had to address their escalating costs through negotiations with the provincial authorities who themselves had no resources designated for that purpose.45
18 In 1958, after the department of health consulted with the Union of Nova Scotia Municipalities, a set of provincial standards was presented to the managers of the 15 remaining municipal mental hospitals.46 Institutions which could meet, or show evidence of the ability to meet, minimum requirements relating to such matters as administration, records, staffing, building safety and programming were able to qualify for provincial financial assistance. Several inducements designed to secure cooperation were included: 1) what seemed like generous funds to establish two tuberculosis units for mental patients (in 1957, a total of 154 active or suspected cases were found in 12 of the hospitals); 2) provision, free of charge, of the now indispensable anti-psychotic drugs along with a training course at the Nova Scotia Hospital on their administration (held on 12 January 1958); 3) provincial funds to cover one-third of a hospital’s operating expenses (increased in 1962 to one-half); 4) consultation services in psychiatry and nutrition and 5) assistance with in-service psychiatric training programmes for all levels of staff.47 Of the nine hospitals that tried to qualify for provincial assistance, four succeeded, including the HCH. The HCH was also one of the two mental hospitals cajoled into accommodating a provincial tuberculosis unit for the insane. This unit proved to be an expensive liability but also, until it was removed in 1966, a short-term bargaining chip for the hospital in its relations with the province.48
19 The 1950s also saw the beginnings of serious volunteer work at the HCH as the mental health movement spread across the province. The Dartmouth branch of the Canadian Mental Health Association (CMHA), established in 1957, initiated a ten-year period of expanded activities culminating in the establishment of the hospital’s own auxiliary to organize activities and coordinate visits by the organization’s "White Cross" volunteers as well as by service, church and youth groups.49
Modernization at the HCH (1959-65)
20 The involvement and influence of key individuals cleared the way for modernization at the HCH in the early 1960s. Prominent among them were two new municipal councillors, Eileen Stubbs, a registered nurse, and Percy Baker, a businessman. Both were elected to the county council at the end of the 1950s. In 1959 Councillor Stubbs made an unexpected visit to the hospital and, not liking what she saw, reported her concerns to the press. Both she and Baker, a man with a mission when it came to the mentally ill, were soon appointed to the hospital’s board. Baker served as chair of the board from 1961 to 1971 and as hospital administrator himself from 1971 to 1984. Stubbs was a relentless crusader for transparency and efficiency until she left the county to enter politics in the new city of Dartmouth in 1961. She often returned to the HCH, however, to visit and became a member of the board again briefly in 1972 before being elected mayor of Dartmouth in 1973. One of Stubbs’ first moves was to ensure that procedures at the HCH were scrutinized by the commission of inquiry into Halifax municipal administration, which she instigated in 1960.50 While the commission’s report blamed the municipal staff more than the hospital for the financial division of authority between the municipal clerk and the hospital’s business manager – a situation which had forced Superintendent Smith to borrow from the patients’ trust funds – a combination of this investigation and revelations of various recent instances of mistreatment of patients increased the pressure for reforms in administration, staffing and therapy.51 Another significant event, which occurred when Smith saw the writing on the wall and retired early, was the appointment of Eric Davies as the third superintendent in 1959. According to Stubbs, Davies, a lay administrator from the Douglas Hospital in Verdun, "brought the Hospital out of the dark ages".52
21 Eric Davies introduced modern psychiatric practices including some freedom for patients through open wards and leaves as well as the promotion of rehabilitation and return to the community. This new flexibility, derived from contemporary "milieu therapy", owed something to Marshall’s support.53 In accordance with Marshall’s mental health policy, the hospital also proceeded with the classification of patients.54 The shift from a dual-purpose institution to an active-treatment centre involved classifying elderly and physically disabled people as sane in order to transfer them to community care or to welfare homes (homes for special care and nursing homes, including Ocean View Home in Eastern Passage, which was established as Halifax County’s principal welfare facility for former HCH patients), and certifying as quickly as possible all of the others in order to retain a patient load in the HCH which was financially viable.55 The driving force behind these developments was the Social Assistance Act which brought federal funds into Nova Scotia for cost-sharing the care of the elderly and disabled poor. Within two years of Davies’ appointment, the hospital benefited from better salaries, in-service training, conference and course travel for staff, adoption of revised personnel policies, appointment of a part-time director of volunteers paid for by the CMHA, reform of the pastoral care services and, at Marshall’s request, closure of the dreary staff quarters.56 In 1962, despite the institution’s continued staffing problems and complete lack of psychiatric specialists, Marshall – still adept at damning with faint praise – assured the board that the HCH was "certainly the best County Hospital in the Province".57
22 A sincere commitment to rehabilitation combined with the effectiveness of the new generation of drugs resulted, in 1962, in the first placement of patients in foster homes or family care.58 Unfortunately, Kevin Burns, the hospital’s first social worker, who found placements for rehabilitated patients, was lost to a better-paying job in 1964 and HCH was without a replacement for five years.59 In the interim, municipal welfare officers assumed responsibility for the external aspects of truncated rehabilitation and community residence programmes. In the hospital itself volunteers – mainly well-educated, middle-class women – contributed to the programme by acting as stopgap occupational therapists and social workers. The role of chaplain continued to grow in importance as counselling by professionals, including non-medical ones, became an accepted practice in mental health circles. When the Protestant part-time chaplain died in 1965, the superintendent suggested the replacement should not only be interested in mental health but also be "a Christ-like man who knows these people are sick and cares for them as they are" and "be able to meet patients on their own level and converse at this level".60
23 The hospital was not so fussy when it came to psychiatrists: any qualified psychiatrist would do. The acquisition of adequate psychiatric help involved many false starts.61 In 1963 the board finally induced a very experienced, highly regarded, retired government psychiatrist from Ontario, Dr. Daniel O’Gorman Lynch, to take a part-time appointment, but the medical staff was still too small to do even the most routine examinations.62 Dr. Malcolm estimated in 1966 that, with the available services, it would take one year to give a physical examination to every patient and two-and-one-half years to give every patient a psychiatric evaluation.63 At the same time, the introduction of intensive, personalized therapies increased the workload and the level of responsibility of an already over-extended nursing staff. Nurses also required a higher level of training of a more specialized nature to deliver these treatments effectively. It was clear that the hospital would have to provide inexperienced nursing staff with in-service training in psychiatric care. Davies was able to improve the salaries of the graduate nurses by adopting the scale recommended by the Registered Nurses’ Association, which meant that by 1965 "the Hospital was obtaining a better calibre of staff members".64 That same year a new director of nursing was appointed – the first man to hold the position – who had some experience with British social psychiatry from which the HCH began to draw its inspiration.65 Leslie Havers, who had most recently worked in Ontario, got on very well with Eric Davies, the superintendent. Perhaps not surprisingly, however, these newer administrators, recruited from central Canada, met with some resistance from the older, long-established medical and nursing staff.66
24 While much of the interest in patients displayed by administration and management related to preparing them for independent living in community settings, the most chronic "lifers" also enjoyed greater variety in their institutional lives. Some of the men who needed the hospital’s help on a continuing basis were allowed to go out to work by the day; for others who worked within the hospital, both men and women, a wage scale (instead of the previous standard gratuity) was developed to encourage various levels of attainment. Social events, including group expeditions off the hospital grounds for bowling, indoor swimming and films, became more frequent, and self-expression was encouraged through such activities as a patients’ orchestra. The hospital’s new recreational and devotional centre opened in 1964. That same year the farm, which had been a source of work "therapy" for a small number of male patients, was discontinued because it cost the municipality more than it returned.67
25 The conversion of the HCH to an exclusively psychiatric facility took far longer than the administration had been led to believe by Marshall. The job of classifying existing patients and the process of removing those eligible for social assistance to facilities run by the department of social services or, as the hospital preferred, to community residences, continued for years. As well, several other "special" populations commanded the attention of the board. The hospital worked unceasingly, often in cooperation with the Canadian Association for Retarded Children, to force the provincial government to remove the "grossly retarded" children to facilities which provided better care. Another major concern was the lieutenant governor’s warrant cases. The plight of fisher Charles Perry, a hermit from Ship Harbour on the Eastern Shore who came to Percy Baker’s attention, is a case in point. Before he was hospitalized, Perry’s neighbours used to amuse themselves at night by parking their cars on a rise overlooking his abode and flashing their headlights on and off at his windows. In response Perry finally wrote a letter of complaint to one of his persecutors accusing her of holding drunken parties. The RCMP advised the recipient to prosecute for intimidation, which she did. When Perry arrived in court armed with his Bible, he called the judge a sinner. Charged with contempt of court, the hapless fisher was declared unfit to stand trial on either of the charges and was "dumped" into the Halifax County Hospital. It took the persistence of his sister and the help of his municipal councillor to secure the eventual lifting of the warrant.68 Not only did the staff and board object to having to confine indefinitely patients for minor infractions of the law – besides Perry’s so-called threats against a neighbour, their offences included stealing "an old telephone" and breaking a window valued at $2 – they also resented being forced to keep them under lock and key.69 Although Davies boldly started to integrate warrant patients into the normal hospital routines in 1963, and the medical staff put pressure on the attorney general’s department for releases, it required new legislation to ensure that such cases would receive regular review. As the next chapter in the HCH’s existence dawned on 1 January 1966 with the proclamation of the Municipal Mental Hospitals Act, the institution remained on the one hand a prison and, on the other hand, a hospital now open to voluntary admissions and one to which, in the interests of patients’ rights, involuntary commitment became more difficult.70
A State of Catharsis at the HCH (1966-70)
26 The fourth phase at HCH presents a far more complicated picture as a result of four developments. First, the majority of patients were drawn from further afield, involving many different jurisdictions, as the smaller and unapproved institutions across the province closed. With only about 20 per cent of the patients now from Halifax County itself, the hospital became more a regional than a strictly municipal institution.71 When some patients appeared to be ready for foster homes, the HCH was confronted for a number of years with the inability of other municipalities in its catchment area (most of the eastern and northern mainland) to provide the social support system essential for placement and follow-up. Second, with the transfer of the children, the "feeble-minded" disabled and the elderly to special care facilities and of the rehabilitated to community care, the patients were now primarily the "very, very disturbed". These circumstances could have resulted in a return to locked wards, a potential development that the medical staff regarded as regressive.72 Third, the administration had to cope with the Nova Scotia Hospital Insurance Commission (NSHIC), a frustratingly bureaucratic and parsimonious taskmaster, which finally assumed responsibility for the hospital in 1966. The new legislation that accompanied the takeover used more politically correct language – the asylum became the mental hospital – and provided more flexibility regarding both admissions and discharges. The commission itself, however, was blind to the urgent problems related to staffing, patients and treatment. Indeed, Dr. Graham Simms, assistant deputy minister of health and executive director of the NSHIC, outraged the HCH board with his dismissive assertion that short-range problems should not be allowed to interfere with the long-range programme. "Long" was always too long for the board.73 Key critics of the mental hospitals tended to concur. In 1967 Dr. R.O. Jones told a parliamentary gathering that "there are too few doctors, fewer nurses and ward attendants and practically no social workers or occupational therapists" in the mental hospitals administered by the NSHIC.74 Fourth, a series of incidents in the late 1960s undermined public confidence in the institution. These included in 1967 a case of brutal treatment of a patient by an attendant, a fatal suicide pact between two male patients, the pregnancy of a promiscuous patient allegedly caused by a hospital worker and, in 1968, a nasty case of brutality and buggery, which led to staff dismissals and criminal charges against an attendant. The resulting poisoned atmosphere encouraged an outraged Chairman Baker and a distressed Superintendent Davies to employ Pinkerton detectives as undercover ward attendants in order to identify other staff engaged in inappropriate activities. Baker also called for a royal commission to look into the operations of the hospital. In response to his request and the concerns of others, the commission convened in 1968 and tabled its final report in 1970.75
27 Throughout the problems of the late 1960s, the rehabilitation programme nevertheless remained on course, although not without considerable disagreement. Havers soon ran afoul of Dr. Malcolm over patient care, procedures for dispensing drugs and, more fundamentally, over the respective roles of the medical officer and the director of nurses. Malcolm disparaged Havers as "only a nurse" and insisted "medical staff had to have control of the nursing staff in any hospital".76 Havers not only disagreed, but also secured the support of the superintendent and, through Davies, the board. As a result, both the chief and assistant medical officers resigned in 1966, although Malcolm recovered sufficiently from the assault on his dignity to do some post-retirement consulting. Malcolm’s reluctant successor as chief medical officer (and clinical director), the young and idealistic Dr. John Barteaux, promoted HCH’s new rehabilitative milieu by expanding the occupational therapy programme to include the physical space of the wards themselves in addition to the dedicated occupational therapy premises.77 This diversification necessitated the in-house training of occupational therapy staff. Since the hospital insurance commission would not pay for the programme until the HCH hired a registered occupational therapist to head it, the search for the elusive specialist – well-qualified occupational therapists in Canada were as scarce as hen’s teeth – continued until Douglas Flock, billed as one of the best practitioners in the country, was recruited from Quebec in 1969.78 The rehabilitation programme included tutoring in social skills, confidence building, practice in cooking and domestic management, and job training. Barteaux’s imaginative approach to rehabilitation is illustrated by the case of Lettice Edwards, whom he characterized as a paranoid schizophrenic. An eccentric, spirited woman from Sable River on the South Shore, Edwards had been committed to the Nova Scotia Hospital in 1953 by her equally eccentric mother. After 14 months and a suicide attempt, Edwards was transferred to the HCH where she languished for the next 12 years while waging a campaign of resistance by firing off some 300 letters requesting legal help in her relentless bid for freedom. None ever left the confines of the hospital where all outgoing mail addressed to public officials was censored. At this point, Barteaux agreed to permit Edwards to take a correspondence course in Canadian business law. Only after she successfully completed her course was she able to use her new knowledge to secure the help of a lawyer and obtain her discharge in 1967.79
28 For patients in transition or for those whose persistent, serious behavioural problems made them unlikely candidates for release into the community in the near future, another programme – the therapeutic community – was established with the intent of redefining patients’ relationships with their caregivers. This approach, pioneered in Great Britain and brought to North America by British-trained social psychiatrists, had been introduced at the Nova Scotia Hospital in the early 1960s. It was adopted in part at the HCH in the late 1960s and included group therapy sessions, the only kind of psychotherapy the hospital could afford. Designed to modify patients’ behaviour by motivating them and giving them more responsibility, patients were involved in a democratic form of problem solving, which included the establishment of a patients’ council and the production of a news-sheet written from their perspective.80 Since employment of patients as labourers in the various hospital departments was not seen to be therapeutic, it was phased out in 1970, at least temporarily.81 The therapeutic community required the cooperation of all staff members, from cleaner to medical officer, each of whom was expected to relate to the patients, as well as to each other, in a democratic and supportive fashion. Authoritarianism was outlawed; hierarchy was disguised. Upgrading the quality of the non-professional staff was therefore considered essential to the success of the programme, but inadequate salaries continued to pose a major problem. Staff complement also remained insufficient, something which the board could now blame on the dilatory hospital insurance commission, which refused to proclaim in a timely fashion a viable staff-patient ratio for the mental hospitals.82 Comparisons with resources available at other hospitals in the system underscored deficiencies at the HCH. For example, in the male maximum security ward at the Nova Scotia Hospital five attendants took care of 14 patients; at HCH there were three attendants for 51 patients.83 For those in charge of the hospital, the lack of an applicant pool for attendants forced them "to hire almost anyone who is willing to work" regardless of qualifications. Even these attendants stayed, on average, only a couple of weeks.84 According to a report in The 4th Estate, "Some of the staff . . . were probably just as sick as the patients".85
29 Because of the shortage and low quality of the staff, the volunteer services department remained a vital component of the hospital. By 1967, 49 different organizations contributed to the programmes supervised by the coordinator of volunteer activities.86 For the non-professional staff, who constituted the majority of employees, arguably the most important development of the 1960s was unionization. The first contract with the Canadian Union of Public Employees was signed in November 1967.87 While the hospital administration welcomed the union as a vehicle for improving the woefully inadequate salaries, it refused to be intimidated by the prospect of grievances, as evidenced by the dismissal of 22 employees, including 15 CUPE members, as part of a zero-tolerance policy in the aftermath of the Pinkerton investigation into the behaviour of staff members during their shifts.88
30 As for the professional staff, it was not until public attention was focused on the hospital’s scandals that Marshall found the funds in 1968 to support more psychiatric services, including a full-time psychiatrist aided by regular part-time assistance from several government psychiatrists. Certainly the constructive critique embodied in the Report of the Royal Commission on the Halifax County Hospital, which had wide-ranging implications for the whole mental health system in Nova Scotia, attracted much-needed resources for the hospital. The number of registered nurses increased significantly and the reliance on unqualified nursing attendants diminished. Indeed, recruitment was so successful that, for the first time in the hospital’s experience, there was a waiting list for attendant positions.89 Under the guidance of an extremely sympathetic commissioner, the Honourable H.P. MacKeen, who had just stepped down as lieutenant governor, tragedy was turned into triumph, as he put it, and the institution seemed to be better prepared to undertake the challenges of the 1970s.90 In the process, however, HCH lost Superintendent Davies, who was scapegoated for the incidents which precipitated the royal commission as well as for undertaking major renovations of the erstwhile "dungeons" or "hell-holes" – ordered closed by Barteaux – without written authorization from the NSHIC. It also lost its reputation as Nova Scotia’s best regional mental hospital and was relegated to third place after the Kings County Hospital, which had a more modern facility at Waterville, and the Halifax Mental Hospital (which was replaced by the new Abbie J. Lane Memorial Hospital in 1971); this left it superior only to the Cape Breton Hospital (see Table).91 With the benefit of hindsight this official downgrading can be seen as a preliminary to the institution’s elimination as a "health" facility. It also made it easier for the government to impose a whopping budget cut in the spring of 1970. As a result, Barteaux and the board feared that, after all the recent improvements, the hospital would be turned into "a boarding house with no psychiatric treatment" and they deplored the financial decisions of "the pencil pushers in the ivory towers".92
31 The therapeutic community concept also lost some of its lustre.93 Staff feared that control of the hospital was shifting to the patients.94 Davies had been opposed to its implementation and so too had the male patients’ new head nurse, Frank Rogers, a first-rate recruit from England with psychiatric training. When Dr. Barteaux found that Rogers, by then director of nurses, would not support Flock’s rehabilitation therapy, he reluctantly had to let the nurse go. Barteaux himself ran up against the NSHIC administrators, who looked askance at a general practitioner assuming authority over psychiatrists in the running of the hospital. Although Barteaux willingly undertook a residency in psychiatry on the basis of his formative experience at the HCH, he found he was unable to continue his hospital duties and maintain control of the programme of care. Like Malcolm before him, he ran into difficulty with the board over lines of authority. As a result, a new medical director for the HCH, Dr. Everett Smith, was found among the psychiatrists at the Nova Scotia Hospital.95 Another blow to the therapeutic community occurred in 1970 when psychiatrist Dr. Wilkie Kushner, chief proponent of the model, who worked part-time at the HCH, realized he was wrong to think that his patients understood the concept of caring for each other. One patient pushed another into the now-fully accessible Bissett Lake on the hospital property, with the result that he drowned.96 Finally, some of the board members had great difficulty in accepting the mixing of the sexes in social activities, which common day rooms encouraged, even if they agreed with Barteaux that it was the patients’ illnesses, not their morals, that must receive priority. They were also offended by the low standard of housekeeping which ensued when patients were allowed to control their own living space.97
The HCH in Limbo (1971-76)
32 The HCH was proud of its pioneering achievements in Nova Scotia: it was the first municipal mental hospital to launch a rehabilitation programme, employ a social worker, pursue community residence for patients and open an unsupervised rehabilitative ward.98 It also spearheaded the movement to establish a programme for severely retarded children and remove them from the mental hospitals to their own dedicated facilities.99 Moreover, by 1975 it was still the only psychiatric hospital in the province to promote and maintain sheltered workshops, which provided a non-threatening environment for people with mental disorders.100 After the events surrounding the royal commission, the hospital benefitted for the first time from a high-quality staff.101 Yet the years between the 1971 and 1976 were ones of great uncertainty for the HCH. Rumours that it was expendable within the mental health system, now presided over by Marshall’s successor, Dr. Ralph Townsend, were unsettling.102 It was just too close geographically to the Nova Scotia Hospital, itself in transition, to be able to maintain its customary role. In the meantime Leslie Havers, Davies’ successor as administrator, committed suicide in April 1971 and was succeeded, somewhat implausibly, by Percy Baker, erstwhile chair of the board and longtime municipal councillor.103 Baker remained in the post for 13 years, thereby overseeing the institution’s change of jurisdiction from health to social services and its new role as the Halifax County Regional Rehabilitation Centre. Baker won people’s admiration by his sheer tenacity – at least as a talker – but his lack of qualifications for the position did not go unremarked. He was a furrier by trade and laundry and dry cleaning specialist by experience and was rumoured to have a grade five or six education. He was certainly astute enough to garner some impressive salary increases for himself and, to silence his detractors, he successfully participated in a hospital management course.104 In 1974 Townsend attributed the hospital’s improvements to Baker, although he found his approach to staff too dictatorial. His concern for the patients’ comforts, however, was genuine. Indeed, as Townsend noted, "while in many ways he represents the old-type hospital superintendent who is paternalistic towards the patients, many of the patients in this institution require that kind of approach as they are retarded and child-like in character".105 Medical director Everett Smith, who did not oppose Baker’s appointment, considered Baker to be a consummate politician and opined that if Baker had been well educated he could have become prime minister.106
33 Douglas Flock remained until 1972 the mainstay of the rehabilitation programme, developing job training and sheltered workshops (carpentry and printing mainly) in both the hospital and the city of Dartmouth. Then, as a result of his accounting practices and aggravating hubris, he ran afoul of Baker and others and was let go. His ensuing lawsuit for wrongful dismissal hung over the board until an out-of-court settlement was reached in 1975.107 Nonetheless, the hospital’s occupational therapy and rehabilitation programmes continued to attract interested and enthusiastic visitors from a number of institutions. In addition, its increasing and enforced association with the Nova Scotia Hospital, which was in the process of becoming a regional chronic care hospital in addition to maintaining its traditional role as the province’s acute care facility, was made more palatable by the favourable comparisons between the levels of their respective expertise in geriatrics and rehabilitation.108 Smith, who was intimately acquainted with both institutions during this transitional period, considered that the chronically ill received much better care at the HCH than at the Nova Scotia Hospital.109 Moreover, the hospital’s clinical staff took a lead in establishing group homes and an associated day-care programme. In the 1970s the HCH received accreditation from the Canadian Council on Hospital Accreditation, a guarantee that it met approved minimum hospital standards.110 The medical staff’s greatest achievement of the period was the opening of the last locked unit for psychotics, the maximum security ward and the discharge of the most "dangerous" of the lieutenant governor’s warrant cases. Considerable coaching was required to prepare intransigent, unsocialized patients for their encounter with the classification committee of the provincial department of social services. That the patients were able to rise to the occasion was evidence of the success of the "reality" therapy and role playing encouraged by Everett Smith, who trained them to present themselves well in order to maximize the likelihood of their being released.111
34 By the early 1970s, the patient population was becoming increasingly male as women were more readily accepted as community residents and as vehicular and industrial accidents caused more brain injuries. Privileges continued to grow as the government became cognizant of patients’ civil rights.112 Restricted visiting hours were ended in 1971 and the operation of a hospital bus to town was scheduled to accommodate patients’ needs.113 Some of the patients even went on camping trips.114 Opportunities for self-expression and cooperation included art competitions, participation in civic celebrations and the provision of schooling. Hospital employment in the various departments was reinstated for patients, and the better adjusted among them were formed into a uniformed escort service to accompany other patients off the hospital grounds. But as psychiatric patients they could never be entirely trusted. Shortly after a new patients’ library opened in 1974 fifty volumes went missing. The piano was kept locked between periods of authorized usage to protect it from abuse. The cutlery was carefully counted before and after meals. Panhandling or loitering in the front entrance of the building continued to be a constant feature whenever visitors appeared.115 Sections of the grounds, especially the lake and the woods, were now declared off limits. For its part, the elected patients’ council seems to have concentrated on trying to improve the food services, always a vital concern of the institutionalized. But even it had to be "re-motivated" from time to time. In 1974, third-year medical students taught by Everett Smith tellingly undertook a project on the "laziness" that institutionalized patients often exhibited.116
35 The psychiatric role of the HCH ended in 1976, although it took time to transfer patients who were considered suitable for treatment back to the Nova Scotia Hospital. The fate of the remaining patients, "post-mentally ill and others who, in addition, are congenitally retarded", was dependent upon the provincial government’s success in finding ways to cost-share the support of its helpless citizens with the federal government.117 In 1975 the province of New Brunswick negotiated as eligible for maintenance under the provisions of the Canada Assistance Plan "mental patients requiring long-term rehabilitation".118 After due study, Nova Scotia also seized this opportunity and the financial responsibility for the HCH was transferred to the social services department – later renamed community services – which continued to operate it as a regional rehabilitation centre until 2002, at which time it was closed.
Epilogue
36 The residents of the HCH were assailed by many demons. Their illnesses were bad enough, but they also found that their most basic human rights were often in jeopardy. In the 1950s married women could not go for drives with their husbands unchaperoned because the administration wanted to avoid inconvenient pregnancies. Patients who went missing were pursued, captured and forcibly returned.119 For most of its history as a mental hospital, the patients’ mail was censored.120 The patients could not rely on the staff to treat them humanely, much to the administrator’s disgust. In response to the executive secretary of the Nova Scotia Federation of Labour, who suggested that an employee dismissed in 1967 for abusing patients should be given a second chance, board chairman Baker denied the request on the ground "that patients do not get the second chance and many of them never get the first chance . . . there is no such thing as second chances when dealing with mental patients . . . we are not talking about pieces of machinery here – but people".121 Even after the transition from a hospital with certified patients to a rehabilitation centre for voluntary residents, the population remained vulnerable to assaults on their citizenship. Shortly before the provincial election in 1978, the Progressive Conservative party attempted unsuccessfully to delete the names of 174 residents from the voters’ list. One of the 174 wrote: "I feel that this was an insult to my intelligence, and my status as a free human being living in a democratic society. . . . There is still such a stigma attached to the term Mental Illness, that it is very difficult for a person who has been treated in a Hospital or Rehabilitation Centre, to break out in the community and try to obtain his self respect, dignity, and return to his former status as a free person who has had some difficulty in the past to cope with the problems that has [sic] occurred in his life".122
37 The common thread that runs through the various phases of the history of the HCH is the grim economic reality posed by penny-pinching municipal and provincial authorities who found it all too easy to ignore the financial needs of an institution that cared for the powerless. Baker repeatedly deplored the low salaries paid to workers and claimed with his typical hyperbole that pay was so low it was "driving young girls to prostitution and young boys to breaking and entering".123 More tellingly, when the minimum wage was first proclaimed in 1965, it affected the income of over 25 per cent of the HCH staff.124 While as a councillor Baker was a party to the financial policies he criticized, he did not hesitate to refer to the county council as "cheap and miserly" when they refused to pay for a recognition banquet for the volunteers on whom the HCH depended.125
38 We would be mistaken if we were to believe that the displays of frustration by Baker and other board members and administrators were contained within the board room and available to us only in the minutes we read as historians. In reality they were part of a deliberate public relations strategy. Until the proceedings of the MacKeen commission were underway, the board meetings of the HCH were routinely open to the press.126 Publicity which placed the HCH in the public eye could have its advantages as well as its disadvantages. On the positive side, government coffers were sometimes opened following publication in the press of the board’s complaints.127 On the negative side, the HCH was, unlike the other hospitals, frequently in the news, making it appear to be the place where suicides, pregnancies, mistreatment and staff problems uniquely occurred. Other institutions tended not to air their dirty linen in public and, as a result, escaped both the rewards and the censure.
39 For the HCH, however, the rewards were few. As most policy analysts – historians and otherwise – have concluded, mental health services have always received the lowest priority when it comes to the allocation of scarce resources, a vulnerability which Clyde Marshall described as being "behind the eight ball".128 Mental health was just not a popular cause. It was not easy to love the chronically crazy. When John Barteaux suggested in 1967 that only 10 per cent of the patients at the Halifax County Hospital had a friend or family member who showed a modicum of interest in their welfare, he underscored a well-known fact that helps to explain the political irrelevance of the insane and the injustices endured by the Lettice Edwardses of Nova Scotia.129 Not only were local patients neglected, but immigrant patients were also ignored. Ivan Trotz’s story of speechless solitude, which became public in 1971, is a case in point. A Russian speaker, he had been a patient at the HCH for 16 years after spending 13 years in the Nova Scotia Hospital. Attempts to deport him as a psychotic alien had apparently failed in the 1940s and it was only when Baker found someone who could speak his language that Trotz was finally, at the age of 71, given a chance to overcome his paranoia after being assured that he would not be returned to the Soviet Union.130 Again and again members of the Canadian Mental Health Association attributed popular perceptions and political neglect to an entrenched stigma that mental illness seemingly could not escape. Shunned by the rest of society, including family members and prospective employers, and repeatedly institutionalized, many chronically mentally ill persons had no means of becoming economically self-sufficient. State functionaries often thought of them as per diem charges under successive pieces of legislation: municipal poor law and mental hospital acts, provincial social assistance and hospital insurance acts, and the federal Canada Assistance Plan. Since only the "curable" were treated under the provisions of the provincial health system, the story of the chronically, seriously mentally ill and the facilities to which they were confined is part of the saga of the welfare system in Nova Scotia.
APPENDIX : Hospital Administration 1940-1976
- Province of Nova Scotia, Department of Health
- Inspector of Humane Institutions
- 1947-1955 J.J. MacRitchie (general practitioner)
- 1955-1968 Clyde S. Marshall (neurologist)
- 1968-1976+ F. Ralph Townsend (psychiatrist)
- Director/Administrator of Mental Health Services Division (initially Division of Neuropsychiatry)
- 1947-1969 C.S. Marshall
- 1969-1976+ F.R. Townsend
- Director of Psychiatric Hospitals, Hospital Insurance Commission
- 1968-1976+ F.R. Townsend
- Inspector of Humane Institutions
- Municipality of Halifax County, Halifax County Hospital management
- Tenders and Public Property Committee 1940-1952
- Welfare Committee 1952-1960
- Board of Management, Halifax County Hospital 1960-1976+
- Chair of the Board
- 1940-1952 W.J. Dowell (county warden)
- 1952-1953 Ross E. Dauphinee (county councillor)
- 1953-1959 P.S. Ferguson (county councillor)
- 1959-1961 Granville Snair (county councillor)
- 1961-1971 Percy S. Baker (county councillor)
- 1971-1976+ Arthur C. MacKenzie (county councillor)
- Halifax County Hospital administration
- Supervisor/Administrator (CEO)
- 1940-1946 J. Frank Smith (municipal home administrator)
- 1946-1959 Edward V. Smith (registered nurse)
- 1959-1969 Eric J. Davies (hospital administrator)
- 1969-1971 Leslie Havers (registered nurse)
- 1971-1976+ Percy S. Baker (municipal politician)
- Chief Medical Officer/Medical Director/Clinical Director
- 1940-1947 Peter O. Hebb (general practitioner)
- 1947-1950 Charles Lamont (general practitioner)
- 1950-1966 Frank Malcolm (general practitioner)
- 1966-1970 John W. Barteaux (general practitioner)
- 1970-1971 Everett A. Smith (psychiatrist)
- 1971-1974 Waheedul Haque (psychiatrist)
- 1974-1976 Everett A. Smith
- Matron/Director of Nursing
- 1940-1945 Mamie Smith (registered nurse)
- 1945-1965 Vera Smith (registered nurse)
- 1965-1969 Leslie Havers (registered nurse)
- 1969-1970 Frank Rogers (registered nurse)
- 1970-1976+ Helen Hemsworth (registered nurse)
- Supervisor/Administrator (CEO)
Notes